Blog Archives

Why Is Circumcision So Popular in America?
This article was published January 5, 2015.
The recent decision by the U.S. Centers for Disease Control and Prevention (CDC) to endorse circumcision as a prophylactic measure against disease has once again drawn media attention to America’s most controversial surgery. In draft guidelines issued in December, the CDC emphasized that the most up-to-date medical science indicates clear health benefits of circumcision—including a 50%-60% reduced risk of female-to-male HIV transmission, a 30% reduced risk of transmission of the human papilloma virus (HPV), and lower risk of urinary tract infections during infancy. On the basis of these data, the CDC is recommending that health care workers counsel uncircumcised adolescent boys and men, as well as the parents of newborn males, on the potential benefits and risks of circumcision. The guidelines are currently undergoing a 45-day review period, during which the CDC is actively soliciting feedback.

According to the CDC, roughly 80% of American men are circumcised.
The CDC guidelines follow similar pronouncements made by the American Academy of Pediatrics (AAP). In 2012, the AAP’s “Task Force on Circumcision” issued a revised policy statement and technical report, which concluded that the health benefits of circumcision outweigh the risks, and argued that the procedure should be reimbursed by insurance.
These recent “favorable” reviews of circumcision by the CDC and the AAP come at a time when peer medical organizations in other Western countries are moving in the exact opposite direction. Medical organizations in England, Canada, Australia, Finland, Denmark, Sweden, the Netherlands, and Germany all oppose routine infant circumcision on medical grounds. Several national medical organizations go further and suggest that infant circumcision constitutes a violation of human rights.
It’s not just on policy matters that the U.S. differs from other nations. The strange truth is that the U.S. is the sole country in the world where a large majority of its male population is routinely circumcised at birth for non-religious reasons. According to the World Health Organization, approximately 30% of the world’s males are circumcised. Of these, most (69%) are Muslim men living in Asia, the Middle East, and North Africa; less than 1% are Jewish men; and the rest (13%) are non-Muslim, non-Jewish men living in the United States.
How did the U.S. come to be so out of step with the rest of the world on this issue? America has a long and peculiar relationship with circumcision, and it is impossible to understand the CDC’s and the AAP’s positions without appreciating that history.
Clean Cut
Circumcision, or removal of the foreskin from the penis, is the most common surgical procedure performed in the United States. More than a million newborn males are circumcised by doctors every year. You might think, given these numbers, that circumcision has sound scientific logic behind it. You would be wrong. In 1971, when the rate of neonatal circumcision in the U.S. was near its peak of around 80-90%, the American Academy of Pediatrics concluded that, “there are no valid medical indications for circumcision in the neonatal period.”
To be sure, various health benefits have been proposed over the years, but none that has ever stuck. In the midst of the latest debate about HIV transmission and other risks, it is easy to forget that circumcision has long been, in America, a cultural practice looking for a medical justification.
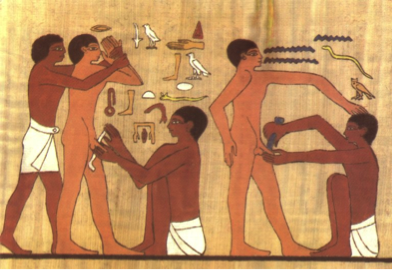
Ritual circumcision has been around forever. The earliest known depiction dates from 2400 B.C. in Egypt. National Library of Medicine.
As medical historian David Gollaher shows in his engaging book Circumcision: A History of the World’s Most Controversial Surgery, the American medical fascination with the procedure can be traced to the enthusiasm of a New York-based orthopedic surgeon named Lewis Sayre. In the 1870s, Dr. Sayre—who would go on to become president of the American Medical Association—developed a theory about the value of circumcision in treating muscle paralysis. The theory depended on the then-popular notion of reflex neurosis, which held that many diseases were caused by persistent stimulation of the nervous system by “irritation.” Dr. Sayre believed that by removing the foreskin he could eliminate one form of this “irritation” and thereby relieve the paralysis. (Interestingly, this was also the basis for removing a woman’s ovaries to combat hysteria and backache.) Sayre’s intervention, which he first performed on a 5-year-old boy suffering from leg paralysis, was the beginning of the American medical appropriation of what had been a primarily religious ritual.
What Sayre began, other physicians continued with gusto. Circumcision was used to treat conditions as varied as asthma, epilepsy, hernia, and indigestion. When reflex neurosis eventually fell out of medical fashion as an explanation for illness, other uses were found for the procedure. Increasingly, doctors said circumcision could prevent a number of conditions, including venereal diseases like syphilis and gonorrhea, masturbation, and cancer.
Integral to this new emphasis on prevention was the emergent germ theory of disease, which linked numerous deadly diseases to microbes. Americans became obsessed with germs during this period, pursuing cleanliness with an almost religious zeal. And in this pursuit, the genitals were found “filthy by association” (89). Smegma, the oily white substance that accumulates under the foreskin in uncircumcised males, was increasingly seen as a source of contamination, and the area itself became a kind of breeding ground for disease. Circumcision, American doctors thought, made patients cleaner (85).

The angel of cleanliness keeping watch at Ellis Island. From Harper’s Weekly (1885). National Library of Medicine.
This obsession with cleanliness was class inflected. At the turn of the century, as millions of immigrants from southern and Eastern Europe poured into U.S. cities, circumcision became one important way that middle class Americans distinguished themselves from poor, dirty immigrants. In fact, Gollaher suggests that it was this meaning of circumcision as a mark of “civilization” that enshrined it in American popular culture (106-107).
That Americans’ germ obsession didn’t simply call for more vigorous cleaning with soap and water, Gollaher attributes to the increasing popularity of surgery as a discipline at the end of the 19th century. The development of antisepsis and anesthesia, “dramatically lowered the threshold for using the scalpel (97),” he notes. With these advances, it became increasingly feasible to prescribe circumcision as a prophylactic measure against disease.
Doctors’ new enthusiasm for prophylactic circumcision notwithstanding, it’s unlikely that the procedure would have ever become routine if it required adolescent boys and men to agree to genital surgery. As Gollaher ruefully notes, “The ultimate popularity of circumcision depended not on convincing normal men to undergo the ordeal of surgery, but on targeting a group of patients who could not object” (100). Infant circumcision proved to be the perfect solution. By 1920, neonatal circumcision performed by doctors in hospitals was standard procedure in America (105).
“The ultimate popularity of circumcision depended not on convincing normal men to undergo the ordeal of surgery, but on targeting a group of patients who could not object.”
The situation in England was similar to that in the U.S. for the first half of the 20th century; Sayre was widely read in England, too. But by World War II, things began to change. After the war, as Britain began creating its system of national “cradle-to-grave” health insurance coverage, the cost-benefit ratio of various medical procedures became a central concern. And, it turns out, circumcision didn’t make the cut. A British doctor, Douglas Gairdner, who reviewed the issue in 1949 found that scientific understanding of the foreskin was woefully inadequate; little research had ever been done on its normal development, including the time it takes for the foreskin to fully separate from the head of the penis and become retractable. This was remarkable, since one of the most common indications for circumcision since the late 19th century had been “phimosis,” or the abnormal adhesion of the foreskin to the underlying glans. Doctors in both America and Britain believed that the foreskin was normally—that is, in healthy infants—separate from the glans at birth; when it was not, circumcision was indicated. But Gairdner discovered that no one had bothered to find out what happened to the foreskin when it was left alone. Contrary to common wisdom, Gairdner found that boys differed widely in the time it took for the foreskin to naturally separate from the glans—anywhere from birth to 3 years. Circumcision as a treatment for so-called “adherent prepuce” before this time was therefore unnecessary. The National Health Service agreed, and in the years following the circumcision rate in Britain fell, from about 33% in 1948 to less than 10% today, with most of those being done for religious reasons.
Things were very different in the United States. Lacking a national heath care system concerned with cost-containment, the U.S. was not forced to conduct similar cost-benefit analyses of circumcision. Health insurance companies were happy to provide reimbursement for the procedure, and doctors were content to continue to collect payments for performing it. Technical innovations also made the procedure simpler, allowing it to be performed by obstetricians rather than by surgeons. As a result, circumcision became even more common.
The neonatal circumcision rate peaked in the U.S. in the late 1960s, at around 80-90%. Since then, the procedure has been slowly declining—in part due to the skepticism of parents who no longer place blind faith in the medical establishment and in part due to the profession’s own writings.
Risks vs. Benefits
In 1971, the American Academy of Pediatrics issued its first policy statement on circumcision, declaring that there were “no valid medical indications for circumcision in the neonatal period.” It issued this same view again in 1975 and 1977. In 1989, the AAP shifted course, finding now that there were some potential benefits of circumcision, including a reduced risk for urinary tract infections, yet still it refrained from recommending routine circumcision of infants. In 1999, the AAP policy statement on circumcision read, “Existing scientific evidence demonstrates potential medical benefits of newborn male circumcision; however, these data are not sufficient to recommend routine neonatal circumcision.”
The AAP’s most recent policy statement, issued in 2012, went further than it had in previous years, arguing that the health benefits of newborn male circumcision outweigh the risks. What happened in the interim to tip the scales? Most important were several influential epidemiological studies conducted in Kenya, Uganda, and South Africa, which showed that circumcision greatly reduced the rate of female-to-male HIV transmission. Specifically, the studies showed that the rate of female-to-male HIV transmission was reduced by 50%-60%, from about 2.5% to 1.2%, in areas where HIV transmission occurs mainly through heterosexual sex. Though the AAP still declined to endorse routine neonatal circumcision on the basis of this evidence, it did say that if parents elected to have it performed, then it should be covered by third-party reimbursement.
The AAP’s revised policy statement generated quite a bit of media attention. The big news, judging from the American press coverage, was the impact the AAP’s conclusion could have on reversing what some saw as the “alarming” reduction in the number of circumcisions being performed in the U.S. These advocates predicted a “health-care doomsday” marked by a “steep rise in infections and medical-related spending if circumcision rates continue to fall.” In recent years, 18 states have eliminated Medicaid coverage for routine neonatal circumcision, citing lack of medical justification. What that means in many cases is that poor families who lack private medical insurance, and must pay out of pocket, elect not to have it done. For circumcision advocates, the AAP’s statement provides hope that state Medicaid programs will be forced to cover the procedure and American boys will no longer be denied access to it.
Among circumcision opponents, the AAP report also generated passionate responses, though these seem not to have gotten as much press coverage (to judge from popular matches in a Google search).
Circumcision opponents—which include groups such as Intact America, Stop Infant Circumcision and Doctors Opposing Circumcision—level several different arguments against the procedure. First, they doubt the medical rationale, pointing out, for example, that urinary tract infections in uncircumcised newborns are rare (incidence of 0.7%, according to the CDC), and when they do occur can be treated with antibiotics. They also note that rates of STDs, including HIV, are actually higher in the U.S., where circumcision is very common, than in many countries in Europe, like Sweden, Finland, and Denmark, where it is essentially nonexistent.

While not necessarily disputing the findings of the African HIV studies, circumcision opponents do doubt the relevance of these findings to the American context. In the U.S., most new cases of HIV transmission occur between homosexual men. There is no evidence that circumcision reduces risk of HIV transmission in this population (something that the CDC and AAP freely admit). Moreover, circumcision alone does not prevent HIV transmission to either men or women; condoms are still required for that. Advocating circumcision as a way to curb HIV transmission when the U.S. has both the highest rates of circumcision and the highest rates of HIV infection in the industrialized world strikes many critics as misguided.
What about cancer? The rate of penile cancer is exceedingly rare (just under 1 case in 100,000 men per year in the U.S., which translates into a lifetime risk, for any man, of 0.07%, according to the CDC). Circumcision opponents acknowledge that circumcision does lower a man’s risk of getting the condition. Removing one-third to one-half of the skin of the penis, it turns out, is an effective way to protect against contracting what is, after all, a skin cancer. Nevertheless, performing surgery on newborns to prevent such a rare cancer does not, to opponents, rise to the level of medical justification. As Gollaher notes in his book, “A high percentage of skin cancers eventually develop on the nose. But this has not led physicians to recommend prophylactic rhinoplasties” (145).
The American Cancer Society (ACS) agrees that infant circumcision is not a valid or effective measure to prevent penile cancer. “Although infant circumcision can lower the risk of penile cancer,” the ACS website notes, “based on the risk of this cancer in the US, it would take over 900 circumcisions to prevent one case of penile cancer in this country.”
What’s more, penile cancer is caused by infection with the human papilloma virus (HPV). Though neither the CDC nor the AAP documents mention it, there are safe and effective vaccines to prevent HPV infection. And the vaccines, unlike circumcision, offer strong protection against HPV infection.
The second, and closely related, argument opponents raise is ethical. They argue it is unethical to perform a medically unnecessary operation on a human who is not old enough to consent to it. Because most of the purported benefits of circumcision (with the exception of a reduced risk of UTIs) apply only to sexually active individuals, the decision to circumcise or not can be postponed to when the individual is old enough to decide for himself. Removing healthy tissue from an infant, critics say, represents a violation of the Hippocratic oath: primum non nocere. First, do no harm.
(For their part, circumcision advocates invoke their own ethical arguments, likening not circumcising to not vaccinating.)
To many critics, what is most galling about the CDC and AAP guidelines is that they completely ignore the value of having an intact foreskin. Very little attention is paid to the natural function of the foreskin, or to the foreskin as a source of pleasure. Nor are the risks of the procedure—including partial or complete amputation of the penis—ever properly acknowledged.
“Seen from the outside, cultural bias reflecting the normality of nontherapeutic male circumcision in the United States seems obvious.”
Interestingly, though infant circumcision in the U.S. is now routinely done under local anesthesia, this is a relatively recent development. It was not until 1987 that infant pain was taken seriously by doctors. Before that, anesthesia was rarely used (Gollaher, 136).
A third common critique is to accuse American doctors of cultural bias. When the AAP’s 2012 report came out, pediatricians in Europe and Canada took the opportunity to issue a published response, entitled “Cultural Bias in the AAP’s 2012 Technical Report and Policy Statement on Male Circumcision.” The article, co-authored by 38 physician representative of societies of pediatrics, pediatric surgery, and pediatric urology from 19 countries, argues that the purported benefits of circumcision do not rise to the level of medical justification, and certainly not before someone is old enough to consent. But the authors also make the point that this same evidence has been reviewed by doctors in other parts of the world where the conclusions reached were exactly the opposite of physicians in America. “Seen from the outside, cultural bias reflecting the normality of nontherapeutic male circumcision in the United States seems obvious,” they write.
The AAP responded, essentially accusing their European and Canadian counterparts of being biased in the other direction, owing to the cultural norm of non-circumcision in these regions.
Sometimes the critiques can get quite personal. A published commentary on the AAP report written by the group Doctors Opposing Circumcision accuses the members of the AAP’s Task Force on Circumcision of bias verging on outright corruption. The commentary names several members of the task force and lists their potential conflicts of interest, including strong religious beliefs in favor of the procedure, economic incentive in the promoting it, and, in one case, deriving financial income from a medical practice devoted to treating boys with circumcision-related problems. Lest it go unnoticed, an additional potential source of bias is noted: “It appears that no member of the task force had a foreskin.”
* * *
To anyone interested in learning more about the peculiar history of circumcision in America I heartily recommend Gollaher’s book. It provides a valuable context within which to view the recent controversy over the health benefits of prophylactic circumcision. I’ll leave you with an interesting “thought experiment,” courtesy of Gollaher. Imagine, he says, that circumcision never caught on in America—that it was more like Norway in this respect. Now imagine that at a meeting of the American Academy of Pediatrics a doctor proposes in a talk that the genitals of all baby boys should be operated upon in order to achieve marginally lower incidences of urinary tract infections and perhaps a lower risk of STDs in adulthood. No one in his or her right mind would take him seriously, leading Gollaher to conclude, “If routine medial circumcision didn’t exist today, no one would dare to invent it.”
References
American Academy of Pediatrics Task Force on Circumcision (2012). Male circumcision [Technical Report]. Pediatrics. 130(3). [link]
Centers for Disease Control and Prevention (2014). Recommendations for providers counseling male patients and parents regarding male circumcision and the prevention of HIV infection, STIs, and other health outcomes. [link]
Earp, B. D. (2012). The AAP report on circumcision: bad science + bad ethics = bad medicine. Practical Ethics. University of Oxford. [link]
Earp, B. D. (2014). Do the benefits of male circumcision outweigh the risks? A critique of the proposed CDC guidelines. Frontiers in Pediatrics, in press. [link]
Frisch, M. et al. (2013). Cultural Bias in the AAP’s 2012 Technical Report and Policy Statement on Male Circumcision. Pediatrics. 131;796-800. [link]
Morris, B. J., Bailis, S. A., Wiswell, T. E. (2014). Circumcision Rates in the United States: Rising or Falling? What Effect Might the New Affirmative Pediatric Policy Statement Have? Mayo Clin Proc. 89(5); 677–686. [link]
Svoboda, J. S. & Van Howe, R. S. (2013). Out of step: fatal flaws in the latest AAP policy report on neonatal circumcision. J Med Ethics. Published Online First: doi:10.1136. [link]
World Health Organization/UNAIDS (2007). Male Circumcision. Global Trends and Determinants of Prevalence, Safety and Acceptability. Geneva, Switzerland: World Health Organization. [link]

